On this page
Key Takeaways
- FDA cybersecurity (Section 524B) is necessary but not sufficient. Hospitals and EU regulators ask for four more attestations.
- About 70% of the controls overlap across FDA, SOC 2, HIPAA, HITRUST, and GDPR.
- Done sequentially, the five programs take 18-30 months and re-collect the same evidence four or five times.
- Done in parallel from one control set, the same scope compresses to a single 9-12 month program.
- This guide gives you the framework-by-framework summary, the shared-control crosswalk, and a recommended sequencing plan.
FDA clearance gets you on the market. Hospital procurement and EU regulators decide whether you stay there. This guide is the plain-English overview and crosswalk MedTech innovators need to plan a single, parallel-track compliance program across the five frameworks every hospital-targeting, EU-touching connected device must satisfy.
Talk to a MedTech Compliance Consultant · MedTech Compliance Bundle service →
Part 1 - Why FDA isn't enough
FDA clearance proves your device is safe and effective. It does not prove that your company can be trusted with Protected Health Information, that your cloud is auditable, or that EU patients' data is processed lawfully. Every Health Delivery Organization (HDO) - hospitals, IDNs, large clinic networks - runs an independent security and privacy review on every device and SaMD before they sign a purchase order. Their procurement and InfoSec teams expect:
- SOC 2 Type II for any cloud-connected service or backend the device depends on.
- HIPAA Security Rule evidence and a signed Business Associate Agreement (BAA).
- HITRUST CSF (e1, i1, or r2) for high-volume IDN deals where MyCSF assessments are the standard procurement gate.
- GDPR Article 30/32/35 documentation, DPIAs, and a Data Processing Agreement (DPA) if any EU patient data is processed - including via a hospital partner in the EU.
FDA clearance does not satisfy any of those. Most teams discover this in the middle of their first hospital deal and watch the launch slip a quarter - or two.
Part 2 - The five frameworks at a glance
FDA cybersecurity (Section 524B + Feb 2026 final guidance)
What it is: US statutory requirement that every cyber device 510(k), De Novo, and PMA submission include a Secure Product Development Framework (SPDF) narrative, a Software Bill of Materials (SBOM), threat modeling, security testing, and a postmarket vulnerability and patch plan. Who enforces it: FDA CDRH reviewers via the eSTAR submission template. Missing artifacts trigger Refuse to Accept (RTA). Audience: FDA reviewers and your Notified Body equivalent.
SOC 2 Type II
What it is: AICPA attestation against the Trust Services Criteria (Security, plus optionally Availability, Confidentiality, Processing Integrity, Privacy). Type II covers a 3-12 month operating period. Who enforces it: A licensed CPA firm. The report is shared with hospital procurement, channel partners, and enterprise customers. Audience: HDO security reviewers, channel partners, and enterprise SaaS buyers.
HIPAA Security Rule
What it is: US federal regulation (45 CFR Part 164, Subpart C) that requires administrative, physical, and technical safeguards for electronic Protected Health Information (ePHI). Includes a mandatory risk analysis and a signed BAA with every covered entity. Who enforces it: HHS Office for Civil Rights (OCR). Violations trigger investigations and civil penalties; HDOs require evidence before contracting. Audience: OCR investigators and hospital privacy officers.
HITRUST CSF (e1 / i1 / r2)
What it is: A prescriptive, certifiable controls framework that incorporates HIPAA, NIST, ISO 27001, and others. e1 (Essentials, 1-year) is entry-level; i1 is the intermediate validated assessment; r2 is the full risk-based, two-year certification. Who enforces it: HITRUST authorizes External Assessor firms to perform validated assessments through the MyCSF platform. Audience: Large IDNs and payer customers that mandate HITRUST as their procurement security floor.
GDPR (EU 2016/679)
What it is: EU regulation governing the processing of personal data of EU data subjects. Key obligations include Article 30 Records of Processing (RoPA), Article 32 technical and organizational measures, Article 33/34 breach notification (72-hour DPA notification), Article 35 DPIAs for high-risk processing, and Chapter V international transfer mechanisms (SCCs, adequacy decisions). Who enforces it: National Data Protection Authorities (DPAs) across the EU/EEA. Fines up to 4% of global annual revenue. Audience: EU DPAs, EU hospital DPOs, and any EU partner that signs a DPA with you.
Part 3 - The shared-control crosswalk
Across the five frameworks, the same control areas appear again and again. Build them once, document them once, and map the evidence into each framework's language.
Risk assessment & threat modeling - Primary in all five. ISO 14971 + ANSI/AAMI SW96 patient-safety threat model is the input; SOC 2 risk assessment, HIPAA risk analysis, HITRUST CSF risk register, and GDPR Art. 35 DPIA are the outputs.
Policies & procedures - Primary in all five. One SDLC, change management, incident response, and vendor management policy set, mapped to each framework's policy requirements.
Access control & identity - Supporting for FDA, primary for the other four. Least privilege, MFA, RBAC, joiner/mover/leaver. One control, four attestations.
Encryption (at rest & in transit) - Primary in all five. TLS 1.2+, KMS-backed keys, documented for FDA crypto rationale, SOC 2/HIPAA/HITRUST controls, and GDPR Art. 32 technical measures.
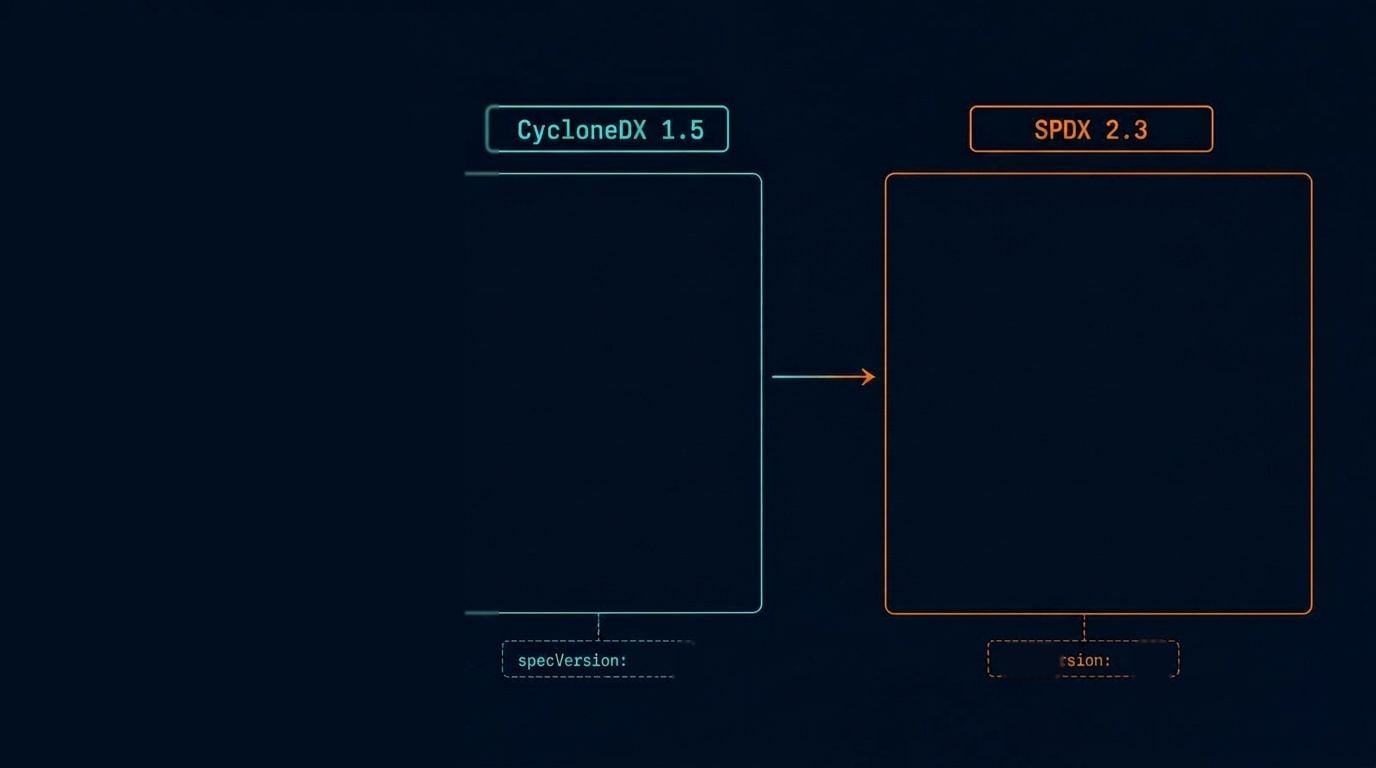
SBOM + vulnerability management - Primary for FDA, SOC 2, and HITRUST; supporting elsewhere. SPDX/CycloneDX SBOM plus continuous CVE monitoring becomes the SOC 2 vuln-mgmt evidence and the HITRUST patching evidence.
Penetration testing - Primary for FDA, SOC 2, HITRUST, and GDPR (Art. 32 testing of effectiveness); supporting for HIPAA evaluation. One white-box test campaign, four pieces of evidence.
Logging, monitoring & alerting - Primary for SOC 2, HIPAA, HITRUST; supporting for FDA and GDPR. Centralized logs with 1-year retention, alerts for security events.
Incident response & breach notification - Primary in all five. One IR runbook covering FDA postmarket reporting, SOC 2 incident process, HIPAA breach notification, HITRUST 11, and GDPR Art. 33/34 (72-hour DPA notification).
Vendor / Business Associate management - Supporting for FDA, primary elsewhere. BAAs, DPAs, vendor risk reviews, and SBOM upstream evidence in one register.
Workforce training & awareness - Supporting for FDA, primary for the rest. Annual security + HIPAA + GDPR training tracked in one LMS.
Postmarket vulnerability disclosure - Primary for FDA and HITRUST; supporting elsewhere. Coordinated VDP and CVE handling required by FDA §524B is reused as the SOC 2/HITRUST vuln-disclosure control.
Data subject rights & Records of Processing - Primary for GDPR; supporting elsewhere. RoPA (Art. 30), data-subject request workflow (Art. 12-22), DPIAs (Art. 35), and SCCs. Doubles as HIPAA right-of-access evidence.
Audit-ready evidence repository - Primary in all five. One evidence vault: FDA eSTAR attachments, SOC 2 fieldwork pulls, OCR/HHS audit, HITRUST MyCSF uploads, GDPR Art. 5(2) accountability records.
Part 4 - Recommended sequencing
Most teams do these sequentially: FDA, then SOC 2, then HIPAA, then HITRUST, then GDPR. Each one re-collects the same evidence and pushes hospital and EU launch out 18-30 months. Run them in parallel from one control set instead.
Months 1-2 - Crosswalk & gap assessment. Map current state to all five frameworks. Produce a single remediation backlog with shared controls flagged.
Months 3-9 - Parallel control build. SDLC, access, encryption, logging, IR, vendor management, training, data-subject rights. Built once, mapped to every framework.
Months 4-9 - Evidence + testing. Threat modeling, SBOM, pen testing, DPIAs, RoPA. Collected once, reused everywhere. SOC 2 Type II observation window starts here.
Months 9-12 - Attestations & submission. FDA cybersecurity submission, SOC 2 Type II audit, HIPAA risk analysis sign-off, HITRUST validated assessment, GDPR Art. 30/32/35 documentation - sequenced to your GTM date.
Part 5 - Five FAQs
Want help running the bundle?
Blue Goat Cyber's MedTech Compliance Bundle runs all five tracks in parallel from one control set, one project manager, one evidence vault, and one fixed fee.