On this page
Published: March 1, 2024 · Last reviewed: May 1, 2026
Key Takeaways
- Microkernels can improve isolation by keeping the kernel small and moving services to user space.
- The security benefit comes from real privilege boundaries, not from the word “microkernel.”
- Tradeoffs include IPC design complexity, performance considerations, and driver ecosystem constraints.
- For FDA-facing evidence, focus on architecture clarity, risk traceability, and verification results that prove isolation and failure containment.
Part of our Medical device security controls, architecture, and integrity primitives series. For the full overview, start with Medical Device Code, Data, and Execution.
Microkernel Architectures for medical devices in 2026: the concrete steps, evidence to capture, and how to align with FDA §524B expectations before submission.
What is a microkernel?
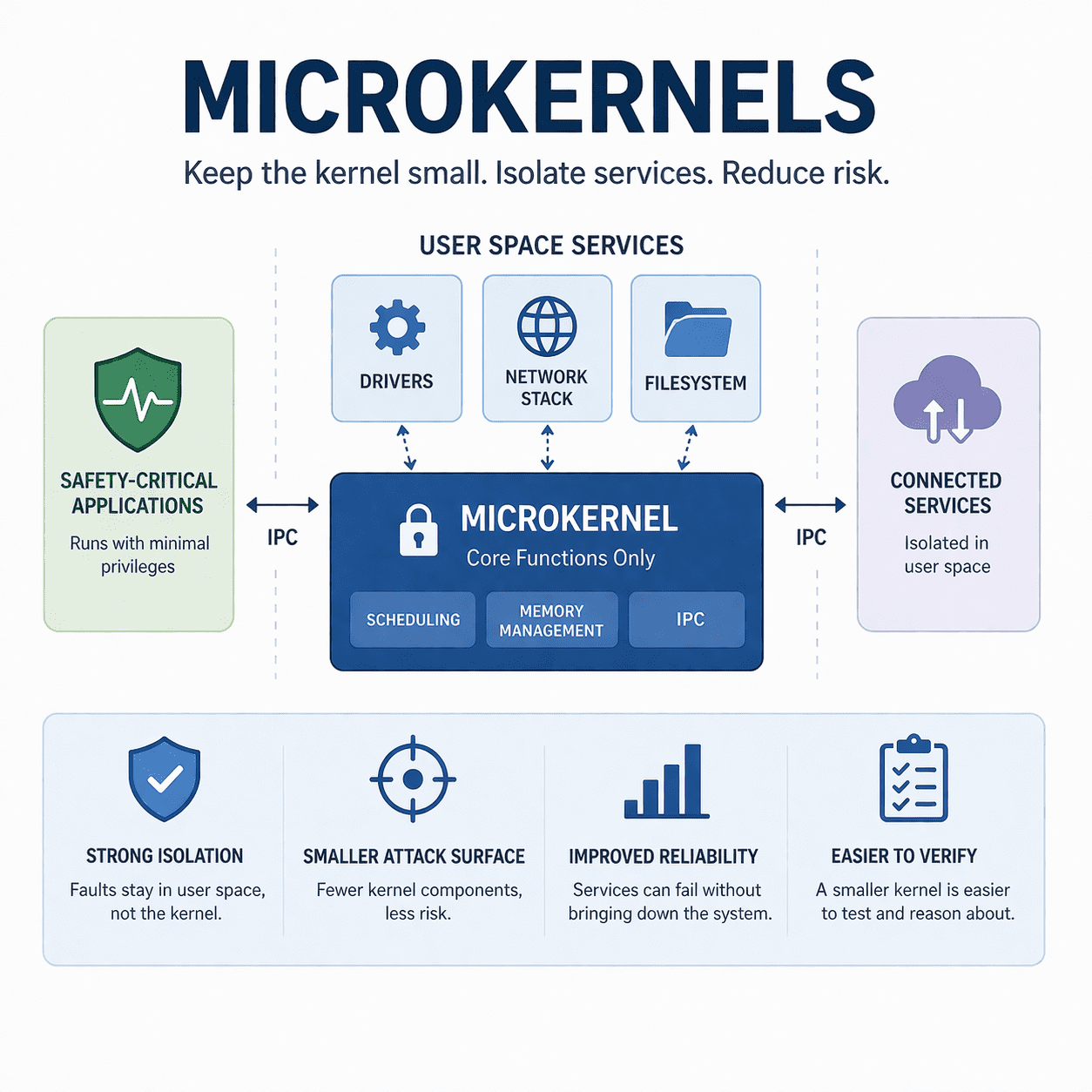
A microkernel is a kernel design that keeps only a small set of core functions in privileged kernel space. Those core functions usually include scheduling, memory management, and inter-process communication (IPC). Other services that would typically live inside a monolithic kernel run in user space as separate processes.
In a microkernel architecture, the OS looks more like a set of cooperating components than one large block of privileged code. The kernel coordinates, user-space services provide functionality, and IPC is the glue.
Microkernel vs monolithic vs “hybrid” kernels
Monolithic kernel (traditional)
Most services run in kernel space. This can be fast and straightforward, but it also means a bug in a driver or subsystem can have a high impact because it runs with full kernel privileges.
Microkernel
Only essential mechanisms stay in the kernel. Many services run in user space with tighter privilege and stronger fault isolation. This can shrink the trusted computing base, but you also introduce IPC design complexity and performance considerations.
Hybrid approaches
Many real-world systems take a blended approach. What matters most is not the label, but where you draw privilege boundaries and how you enforce them.
Why microkernel security matters
In a connected medical device, “cybersecurity” is rarely a single control. It is how you limit the blast radius when something goes wrong. Microkernels can support that goal when you use them to create real isolation between:
- Safety-critical functions (therapy delivery, alarms, essential performance)
- High-risk interfaces (networking, file parsing, removable media, remote service channels)
- Support services (logging, UI, telemetry, update clients)
When the isolation is real, a bug in a non-safety service is less likely to become a full device compromise. That is the value proposition.
FDA’s current premarket guidance emphasizes secure-by-design, architecture clarity, and verification evidence across the lifecycle. If your OS choice is part of your security argument, you should be ready to show how it supports isolation, least privilege, updateability, and vulnerability response. See the FDA guidance here: FDA: Cybersecurity in Medical Devices (Premarket Guidance).
Where microkernels show up in safety-critical systems
Microkernel ideas have a long history in safety-critical domains. A few commonly cited examples include seL4 (known for formal verification work) and QNX Neutrino (known for message-passing architecture in embedded systems). If you want to go deeper on these reference implementations:
- ACM: seL4 formal verification overview
- QNX docs: Microkernel and message passing
These are examples, not recommendations. The right OS for your device depends on your architecture, safety case, maintenance plan, and ability to produce evidence.
The tradeoffs MedTech teams need to understand
1) Performance and latency
Microkernels rely heavily on IPC. That can introduce overhead, especially if services are chatty or poorly partitioned. In many embedded systems the overhead is manageable, but you still need to measure it and make sure it does not affect essential performance.
2) Complexity moves, it does not disappear
A microkernel reduces kernel complexity, but pushes more functionality into user-space services. That can be great for isolation, but it creates more components, more interfaces, and more integration testing.
3) Driver ecosystem and hardware support
Device drivers are often where risk lives. Microkernels can help by running drivers in user space, but only if your platform and vendor ecosystem support that cleanly.
4) Security depends on policy, not architecture diagrams
See also: When to Start Medical Device Cybersecurity, CVSS 3.1 vs 4.0 for Medical Devices: Safety & Automatable Metrics, and Hire Cybersecurity Consultant vs. In-House.
“We use a microkernel” is not a control. The controls are the actual enforcement mechanisms: capability or permission models, memory protection, IPC authorization, secure boot, signed updates, logging, and response procedures.
A practical microkernel security checklist for medical devices
Design
- Partition intentionally: identify safety-critical functions and isolate them from networking and parsing surfaces.
- Define trust boundaries: document which components are trusted, which are exposed, and what happens if each fails.
- Least privilege: ensure each service runs with only the permissions it needs.
- Harden IPC: treat IPC endpoints like APIs. Authenticate and authorize requests between components where applicable.
Build and configure
- Secure boot and secure update: make it hard to persist in the device even if a service is compromised.
- Memory protections: turn on platform hardening (ASLR/DEP or equivalents) where supported.
- Logging that is usable: log security-relevant events, privilege failures, and update events with enough fidelity to investigate issues.
Test and prove it
- Negative tests: prove components cannot access resources they should not access.
- Fault injection: crash or degrade non-safety services and show the safety-critical path stays safe.
- Interface testing: fuzz or stress parsers and IPC endpoints for robustness.
- Security testing: validate exploitability assumptions, not just functional behavior.
If you want support building this into your design process, Secure MedTech Product Design Consulting and Medical Device Threat Modeling Services are designed for exactly this kind of architecture and evidence work.
What to document for FDA-facing credibility
FDA reviewers typically respond well to clear, testable architecture narratives. For a microkernel-based design, your documentation set should make these points obvious:
- Architecture views: partitions, privilege boundaries, IPC flows, update paths, and trust boundaries.
- Risk management linkage: threats tied to components and interfaces, plus mitigations and residual risk rationale.
- Third-party software story: what you run, how you track it, and how you keep it updated, ideally supported by an SBOM.
- Verification evidence: tests that prove isolation, least privilege, and failure containment.
- Postmarket plan: monitoring, patch delivery, and vulnerability response over the lifecycle.
Helpful internal resources:
- FDA Premarket Cybersecurity Services
- FDA-Compliant SBOM Services for MedTech
- Medical Device Cybersecurity Penetration Testing
- FDA Postmarket Cybersecurity Services
- FDA Medical Device Cybersecurity 2026: 524B eSTAR Checklist
Why microkernels matter for medical device cybersecurity
Microkernel architectures are showing up in more safety-critical medical devices because reviewers increasingly want to see the smallest possible Trusted Computing Base behind every life-supporting function. The FDA's Cybersecurity in Medical Devices final guidance dated February 3, 2026 calls out architecture choices that reduce attack surface as evidence of a mature Secure Product Development Framework, and AAMI TIR57:2016 explicitly recommends privilege separation and component isolation as risk-control measures. Formally verified microkernels like seL4 (the only OS kernel with a machine-checked proof of functional correctness, originally completed in 2009 by NICTA/Data61) and Common Criteria EAL 6+ kernels like INTEGRITY-178B carry submission weight a monolithic Linux kernel cannot match. For a Class III implantable or any device touching life-supporting therapy delivery, the choice between a microkernel and a general-purpose OS is increasingly a cybersecurity claim you will be asked to defend in deficiency review.
How Blue Goat assesses microkernel-based medical devices
Blue Goat Cyber tests microkernel-based medical devices the way reviewers expect them to be tested: per-component, against the IPC boundaries, with privilege escalation and supply-chain attacks modeled explicitly. We review the kernel configuration, IPC policies, capability assignments, and any user-space drivers; pen-test the device against the AAMI TIR57 and SW96 threat model; and trace findings back to specific Section 524B(b)(2) requirements in the FDA's Cybersecurity in Medical Devices final guidance dated February 3, 2026. Our testers hold CISSP and OSCP credentials and include ex-military red team operators with embedded-systems backgrounds. Reports cite EAL-rated microkernels (seL4, PikeOS, INTEGRITY-178B) where applicable and document why the architecture reduces the attack surface a reviewer is going to ask about. See medical device penetration testing. If the FDA raises cybersecurity deficiencies after our submission, we resolve them at no additional cost.
FAQ
Are microkernels “more secure” than monolithic kernels?
They can be, because a smaller trusted computing base and stronger isolation can reduce blast radius. But the real outcome depends on how you partition services, enforce privilege, harden IPC, and maintain the system over time.
Does the FDA require a microkernel for connected medical devices?
No. The FDA expects reasonable assurance of cybersecurity based on risk. You can meet that expectation with different architectures if you can document and verify your controls.
Do microkernels eliminate the need for secure coding?
No. You still need secure coding, testing, and vulnerability management. A microkernel can limit impact of a bug, but it does not prevent bugs.
How do we prove isolation in testing?
Use negative tests for privilege boundaries, fault injection to show safety-critical paths remain safe, and targeted security testing for exposed interfaces and IPC flows.
What is the biggest mistake teams make when adopting a microkernel?
Assuming the architecture alone provides security. The hard work is in the permission model, IPC controls, update and logging design, and evidence that those controls work.
Book a Discovery Session
If you want help deciding whether a microkernel approach supports your device’s safety and cybersecurity goals, and you want documentation and test evidence that reviewers can follow, we can help.
Conclusion
Microkernels are a useful tool for safety-critical systems because they can make isolation more practical. In MedTech, the smartest way to use that advantage is to design around trust boundaries, enforce least privilege, test failure containment, and document the results. That combination tends to stand up well in both engineering reality and regulatory review.
Related: The Rising Tide of Cyber Threats in Medical Devices: Understanding the Risks
About the author

Christian Espinosa, MBA, CISSP · Founder & CEO, Blue Goat Cyber
U.S. Air Force Academy graduate and veteran with 30+ years in cybersecurity. Founded Alpine Security in 2014 (acquired 2020), then Blue Goat Cyber in 2022. Has supported 250+ FDA medical device submissions; no client has failed to clear due to cybersecurity. Author of three books including The Smartest Person in the Room. Ironman triathlete and mountaineer.
Sources & references
Primary sources cited in this article. Links open in a new tab.