Cybersecurity guides for MedTech teams.
Practical playbooks, checklists and decoders we use on every engagement.
92 guides

10 Reasons Cybersecurity Vendors Fail MedTech
Why generic IT-security vendors keep blowing FDA submissions - and what to demand from a true MedTech specialist.
Read the guide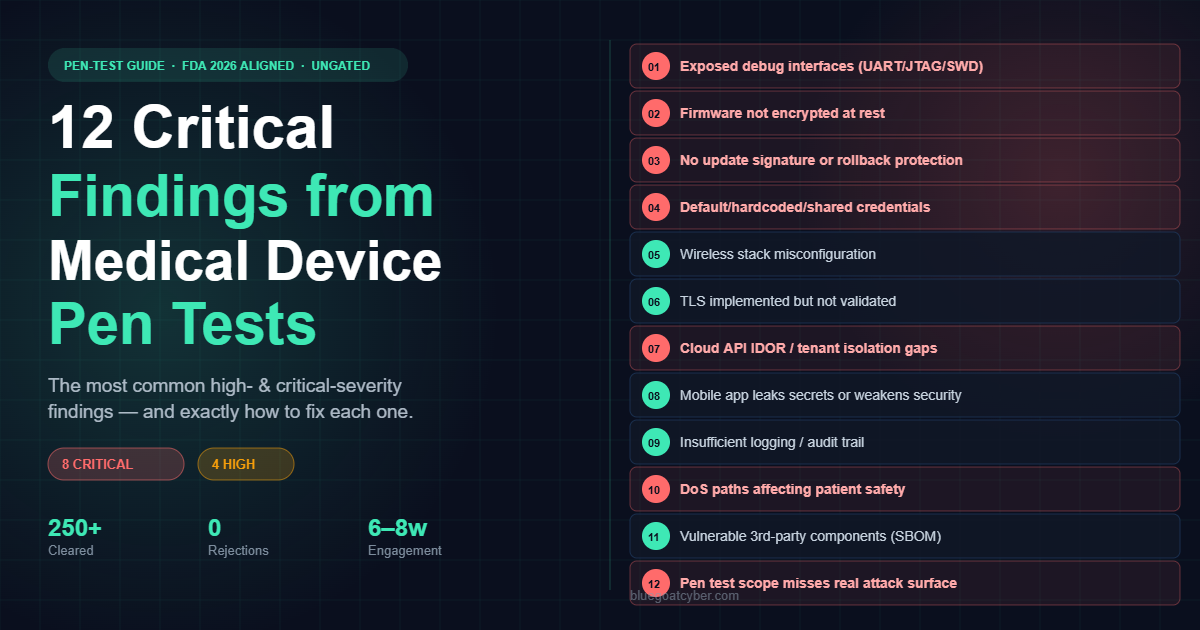
12 Critical Findings from Medical Device Pen Tests
Real, recurring vulnerabilities we uncover during penetration testing on Class II/III connected medical devices.
Read the guide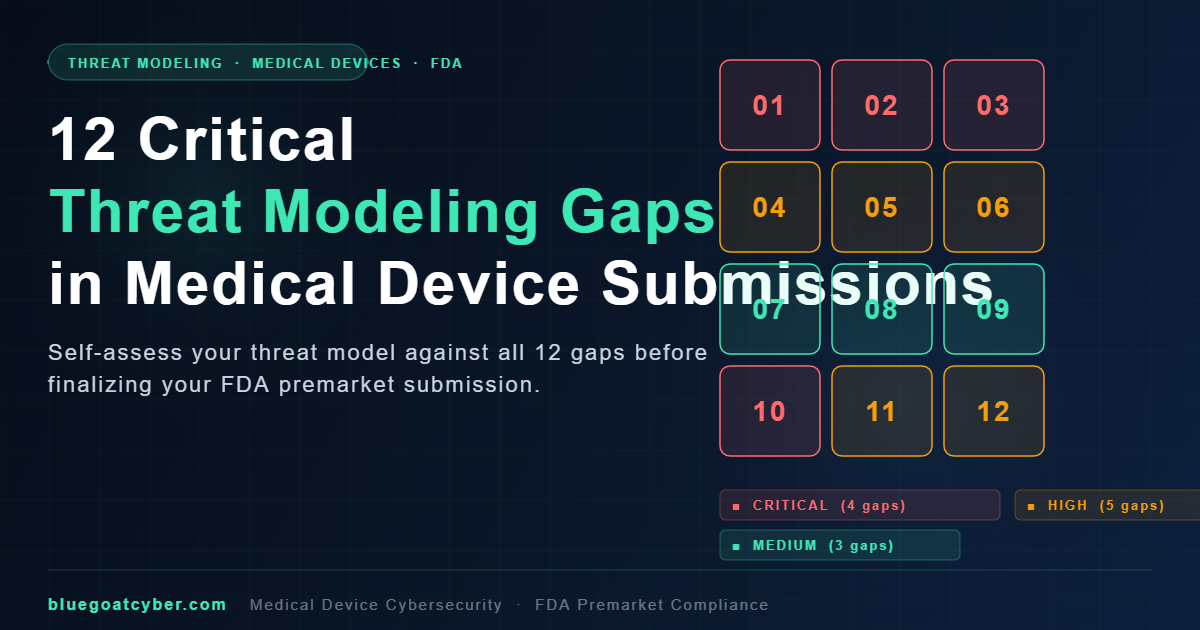
12 Critical Threat-Modeling Gaps in Submissions
Where threat models fall short of FDA expectations under the 2026 cybersecurity guidance - and how to fix the gaps.
Read the guide
12 Reasons the FDA Rejects Cybersecurity Submissions
The most common deficiencies we see in 510(k), De Novo, and PMA cybersecurity packages - and how to avoid each one.
Read the guide
AAMI CR34971 Explained: AI Risk Management for Medical Devices
What CR34971 adds on top of ISO 14971, the AI-specific risk categories it covers, and how to integrate it with your existing risk file.
Read the guide
AAMI TIR57 vs TIR97: Medical Device Risk Management Guide
Compare AAMI TIR57 vs TIR97. Learn how these cybersecurity risk management standards differ and how to apply them for FDA premarket and postmarket compliance.
Read the guide
Board-Ready Cybersecurity 1-Pager + Pre-Read
Board-Ready 1-Pager + Pre-Read Pack When the board asks 'are we covered on cyber?', this is the answer in one page.
Read the guide
Budget-Aware Engagement Structures
250+ 0 6–10 wk FDA submissions supported Cybersecurity rejections Class II eSTAR cyber pack SINCE 2014 TRACK RECORD TYPICAL TIMELINE
Read the guide
Cloud-Only MedTech Threat Surface Map
250+ 0 6–10 wk FDA submissions supported Cybersecurity rejections Class II eSTAR cyber pack SINCE 2014 TRACK RECORD TYPICAL TIMELINE
Read the guideBring this rigor to your next submission.
Book a 30-minute strategy session and we'll map the guides to your actual device, timeline and gaps.